FEVER WITH ABDOMINAL LYMPHADENOPATHY IN A MALE
A 48 yrs old male patient by occupation carpenter belongs to lower middle socioeconomic status came to the hospital on 16/4/19 with chief complaints of
HIGH GRADE FEVER FOR 3 MONTHS,
DECREASED APPETITE FOR 3 MONTHS,
WEIGHT LOSS FOR 3 MONTHS
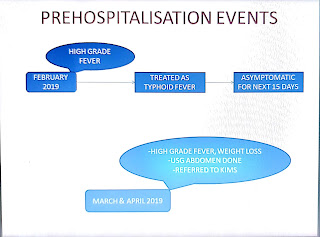
Patient was apparently asymptomatic 3 months back, then in February he developed fever which was of high grade , intermittent in nature , associated with chills and rigors , relieved on medication. This continued for 2 days after which he went to a quack who treated him as having Typhoid fever with medications for 1 week.
This fever was not a/w Burning micturition, ear pain, headache, rashes, generalised body pains, cough, cold, sorethroat,chest pain,palpitations,swelling of both lower limbs.
With this the patient didnt have any fever episodes for the next 15 days. During this period the patient continued to have alcohol daily.
After 15 days he had another episode of High grade fever. The patient was sent to a doctor this time in view of High grade fever and Weight loss. Here he was evaluated, given Iron and Vitamin supplementations and was referred to us.
Outside evaluation showed Raised ESR(130mmhr), Hb(6.9gm%) and Widal positive.

He presented to us with the above chief complaints. He had similar fever episodes as in February.
This man has reduce appetite since 3 months.
History of loss of weight—previously 55kgs now 49 Kgs in just 3 months and not a/w night sweats, Bone pains.
History of Early satiety present since 2 months.
Abdominal pain since 3 months from the xiphisternum to umbilical region ,colicky pain not associated with loose stools or constipation , melena , haematemesis, blood in stools.
PAST HISTORY
Not a known case of Hypertension, Diabetes, CKD, CAD, CVA, Epilepsy, Asthma, Pulmonary kochs.
No history of any surgeries in the past.
No history of any blood transfusion.
FAMILY HISTORY- Insignificant
PERSONAL HISTORY -
Mixed diet
Reduced appetite
Bowel and bladder regular
Sleep adequate
Addictions-
CHRONIC ALCOHOLIC SINCE 28 years(Consumes about 180ml per day of alcohol per day)
He chews Gutka daily.
GENERAL EXAMINATION-
Pallor present
Inguinal Lymph Node: Bilaterally Palpable
Right: 1 cm in size, rounded, firm in consistency, non-tender, no pain on consuming alcohol, matted
Left: Less than 1 cm, rounded, firm in consistency, non-tender, no pain on consuming alcohol, discrete.
VITALS
Temp- 102F




Pulse - 120bpm, regular on right radial artery, Normal volume
BP - 120/70mmhg in supine posture on both arms
RR- 18cpm
Sp02- 98% on room air
GRBS- 110mg/dl
PER ABDOMEN -
On Inspection: fullness was noted in the epigastric region.
On palpation: there is a mass in the epigastric and umbilical region, firm in consistency.
Non tender.
On Percussion: No shifting dullness present.
On auscultation: Bowel sounds heard.
CVS- S1S2 heard, No murmurs
RS- Bilateral air entry present, Normal vesicular breath sounds.
CNS- HMF Intact, No focal neurological deficit.
Genital system- Scrotum normal
Further evaluation was done and following are the reports-

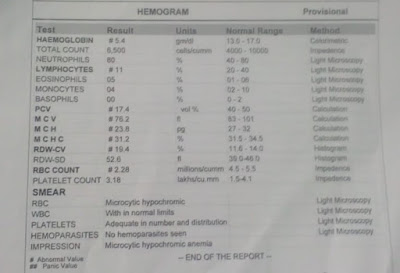
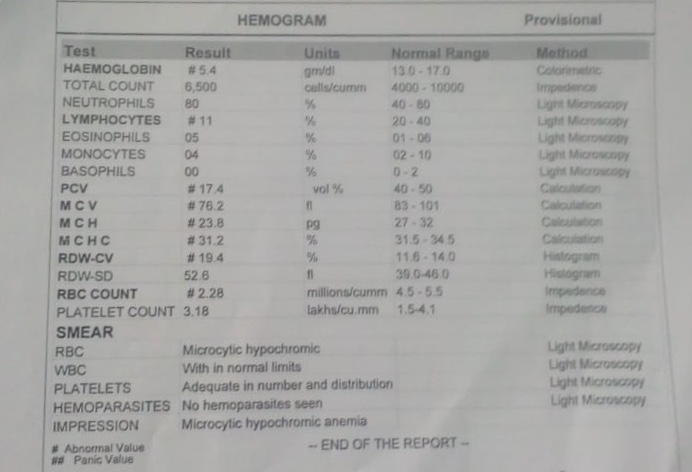
REPEAT CBP:


BONE MARROW BIOPSY WAS DONE.


SCANNER VIEW OF BONE MARROW- LAMELLAE OF BONE MARROW SEEN. LOTS OF FAT SPACES AND HYPERCELLULARITY




USG SCROTUM






CT GUIDED LYMPH NODE BIOPSY WAS DONE
+

LOW POWER: SPECIMEN SHOWING LYMPHOCYTIC SHEETS

HIGH POWER : SHEETS OF LYMPHOCYTES WITH PROLIFERATIVE VESSELS

SURGICAL ONCOLOGIST OPINION TAKEN

MEDICAL GASTROENTEROLOGIST OPINION SOUGHT FOR UPPER GI ENDOSCOPY AND COLONOSCOPY


GENERAL SURGERY REFERRAL WAS TAKEN FOR EXCISIONAL BIOPSY
EXCISION BIOPSY OF RIGHT INGUINAL NODE PLANNED.

MEDULLA AND CORTEX. NORMAL LYMPH NODE
CT GUIDED LYMPH NODE BIOPSY WAS REPEATED AND REPORTS ARE AWAITING.
PROVISIONAL DIAGNOSIS:
HIGH GRADE FEVER FOR 3 MONTHS,
DECREASED APPETITE FOR 3 MONTHS,
WEIGHT LOSS FOR 3 MONTHS

Patient was apparently asymptomatic 3 months back, then in February he developed fever which was of high grade , intermittent in nature , associated with chills and rigors , relieved on medication. This continued for 2 days after which he went to a quack who treated him as having Typhoid fever with medications for 1 week.
This fever was not a/w Burning micturition, ear pain, headache, rashes, generalised body pains, cough, cold, sorethroat,chest pain,palpitations,swelling of both lower limbs.
With this the patient didnt have any fever episodes for the next 15 days. During this period the patient continued to have alcohol daily.
After 15 days he had another episode of High grade fever. The patient was sent to a doctor this time in view of High grade fever and Weight loss. Here he was evaluated, given Iron and Vitamin supplementations and was referred to us.
Outside evaluation showed Raised ESR(130mmhr), Hb(6.9gm%) and Widal positive.

He presented to us with the above chief complaints. He had similar fever episodes as in February.
This man has reduce appetite since 3 months.
History of loss of weight—previously 55kgs now 49 Kgs in just 3 months and not a/w night sweats, Bone pains.
History of Early satiety present since 2 months.
Abdominal pain since 3 months from the xiphisternum to umbilical region ,colicky pain not associated with loose stools or constipation , melena , haematemesis, blood in stools.
PAST HISTORY
Not a known case of Hypertension, Diabetes, CKD, CAD, CVA, Epilepsy, Asthma, Pulmonary kochs.
No history of any surgeries in the past.
No history of any blood transfusion.
FAMILY HISTORY- Insignificant
PERSONAL HISTORY -
Mixed diet
Reduced appetite
Bowel and bladder regular
Sleep adequate
Addictions-
CHRONIC ALCOHOLIC SINCE 28 years(Consumes about 180ml per day of alcohol per day)
He chews Gutka daily.
GENERAL EXAMINATION-
Pallor present
Inguinal Lymph Node: Bilaterally Palpable
Right: 1 cm in size, rounded, firm in consistency, non-tender, no pain on consuming alcohol, matted
Left: Less than 1 cm, rounded, firm in consistency, non-tender, no pain on consuming alcohol, discrete.
VITALS
Temp- 102F





Pulse - 120bpm, regular on right radial artery, Normal volume
BP - 120/70mmhg in supine posture on both arms
RR- 18cpm
Sp02- 98% on room air
GRBS- 110mg/dl
PER ABDOMEN -
On Inspection: fullness was noted in the epigastric region.
On palpation: there is a mass in the epigastric and umbilical region, firm in consistency.
Non tender.
On Percussion: No shifting dullness present.
On auscultation: Bowel sounds heard.
CVS- S1S2 heard, No murmurs
RS- Bilateral air entry present, Normal vesicular breath sounds.
CNS- HMF Intact, No focal neurological deficit.
Genital system- Scrotum normal
Further evaluation was done and following are the reports-

REPEAT CBP:


BONE MARROW BIOPSY WAS DONE.



HIGH POWER: INCREASED FAT SPACES. DECREASED MYELOID AND ERYTHROID SERIES.

PICTURE SHOWING PLASMA CELL

PICTURE SHOWING MEGAKRAYOCYTE

USG SCROTUM


USG LYMPH NODE

CECT ABDOMEN

MEDICAL ONCOLOGIST OPINION WAS TAKEN


+

LOW POWER: SPECIMEN SHOWING LYMPHOCYTIC SHEETS


SURGICAL ONCOLOGIST OPINION TAKEN

MEDICAL GASTROENTEROLOGIST OPINION SOUGHT FOR UPPER GI ENDOSCOPY AND COLONOSCOPY


GENERAL SURGERY REFERRAL WAS TAKEN FOR EXCISIONAL BIOPSY

EXCISION BIOPSY OF RIGHT INGUINAL NODE PLANNED.

MEDULLA AND CORTEX. NORMAL LYMPH NODE
CT GUIDED LYMPH NODE BIOPSY WAS REPEATED AND REPORTS ARE AWAITING.
PROVISIONAL DIAGNOSIS:
-Fever of unknown origin with weight loss, anaemia and abdominal Lymphadenopathy, probably a Non-Hodgkin's luymphoma.
-Unknown infection
-Malignancy with unknown Primary

{kind=link}
His inguinal lymph nodes were not enlarged. In males that is the normal size.
ReplyDeleteMore than 0.5 cm in neck, more than 1.5 cm in axilla and more than 2.5 cm in inguinal would be considered significant